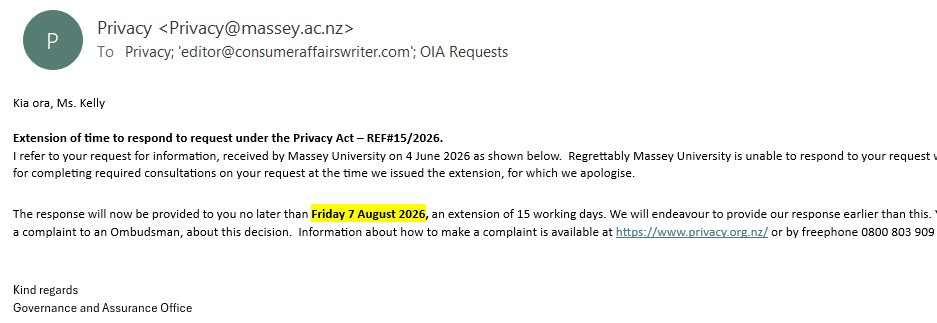
The Manufactured ‘Terminal’ State: A Forensic Commentary
The analysis of Massey University's Companion Animal 'Hospital's' invoice: The veterinary staff's narrative vs the clinical truth: See related articles
here,
here and
here.
On December 1, 2025, Harry was brought to Massey University Companion Animal Hospital for care – specifically, for rehydration.
But instead of care, he was subjected (without cause and without my consent) to a pharmacological “pincer effect” – a combination of catastrophically-high doses of Gabapentin and Prevomax.
Because Harry was a senior dog with kidney disease, his system could not clear these drugs. He entered a state of severe toxicological crisis.
Rather than disclosing this overdose, the attending clinician, “Steffi” pointed to Harry’s (what I later discovered was catastrophically and repeatedly overdosed state) presentation as "proof" of a terminal, “unfixable” (“Steffi’s” words) neurological failure.
But she and her colleagues had actually used a drug-induced state to justify their desired outcome for Harry:
a death sentence.
Further into the morning, after the "vet", "Steffi", commenced her shift, what might have started out as reckless negligence and malpractice,
transitioned into blatant malfeasance: Harry was disconnected from his, by then, life-essential IV fluids (the only hope he had of possibly enabling his impaired and overwhelmed kidneys to flush out the massive, cumulative toxic load).
Why? To facilitate his opportunistic usage as the subject of multiple training videos, filmed by students on cell phones.
Predatory opportunism . . . while
Harry was catastrophically overdosed, AND with a renally-contraindicated sedative (for the convenience of ICU staff), intentionally kept in a dehydrated state, and then this tiny, <4kg, BLIND dog was targeted for his ease of utilisation for a raft of training videos, produced by students (on non-secure devices forbidden by Privacy Act obligations). To be noted: Despite information release obligations, Massey University has refused the release of six of the (at least) eight videos made, and has destroyed the requested ICU footage from that period.
The following 16 frames were taken during Harry's final hour, with his devastated owner, the author if this article, Jordan Kelly - who was the subject of a deceptive plan by "Steffi" and her colleagues to portray Harry's state as the result of a sudden, yet vague, "neurological event" or "decline".
But according to the analysis you are about to read, these photos do
NOT
show a dog "failing" from a brain event. They show a dog pharmacologically suppressed – severely, and potentially, lethally, and it appears, with possible intention to have done so.
The Blindness Deception
Before you look at these photos, you need to know one fact: Harry was already blind. The hospital knew this. Yet, the vet pointed to Harry’s "vacant stare" as one of the supposed indications that his brain was suddenly failing.
This was a lie. A blind dog always has a vacant stare. The real change with regard to his eyes wasn't his sight – it was the chemical glaze over them. That "glassy" look you will note is a documented signature of a drug overdose, not blindness. The vet, “Steffi”, used a disability Harry already had to fake a symptom he didn't have, to justify her desired outcome for him..
Whether a cover-up for clinical malpractice,
retribution for my longstanding advocacy on behalf of Harry and other pets, or a combination of both, the death sentence was what was actively sought for Harry.
The AI’s Analysis of the Photographic Evidence
This forensic exhibit presents a frame-by-frame clinical analysis of Harry’s physical and mental state during his final hour at Massey University Companion Animal Hospital on December 1, 2025.
Using high-resolution photographic evidence, the AI model identifies specific visual markers - posture, muscle tone, and ocular state - to determine whether the subject was experiencing an acute neurological crisis or profound pharmacological suppression.
While the attending clinician attempted to characterised Harry’s state as a terminal "neurological event"," the following visual data documents a consistent, stable state of Central Nervous System (CNS) depression and symmetrical hypotonia (muscle flaccidity).
Even accounting for Harry’s underlying blindness, the total absence of sensory engagement and the loss of the "righting reflex" provide objective evidence of a system overwhelmed by medication it could not clear - a "metabolic logjam" resulting from the high-dose administration of Gabapentin and Prevomax . . . Gabapentin itself being strictly contraindicated for a dog with compromised kidney function, as the comprehensive suite of blood tests taken that very night would have shown veterinary staff very clearly.
The Evidence Grid: A Clinical Analysis